ECR 2017 / C-1585
Neuroendoscopic Third Ventriculostomy : Evaluation of Postoperative Patency and Complications on CT and MRI
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2017
Poster Number:
C-1585
Type:
Educational Exhibit
Keywords:
Outcomes, Diagnostic procedure, Complications, MR, CT, Neuroradiology brain, CNS
Authors:
S. Wassef1, J. Greenlee2, T. Moritani2; 152242, IA/US, 2Iowa City/US
DOI:
10.1594/ecr2017/C-1585
, third ventricular floor (b), aqueduct (proximal portion is enlarged in this case) (c), and suprapineal recess overlays the pineal gland inferiorly (d). Note the suprachiasmatic recess bowing (Bowing sign) on this preoperative MRI (blue arrow).")
Fig. 1:
Anatomy of the third ventricle as seen on 2D turbo spin echo T2WI:
The...
 and 3D CISS sequence (right) in the sagittal plane demonstrating anatomical patency of the ventriculostomy site in the floor of the third ventricle. Note the tectal glioma in this case.")
Fig. 2:
T1 (left) and 3D CISS sequence (right) in the sagittal plane demonstrating...

Fig. 4:
3D SPACE sequence in the sagittal demonstrating prominent flow artifact at the...

Fig. 5:
phase contrast sequence in the sagittal plane demonstrating functional flow...
 and axial CT (right) showing postoperative intra-ventricular hemorrhage and pneumocephalus.")
Fig. 13:
Sagittal 3D CISS (left) and axial CT (right) showing postoperative...
, left (B), and bilateral (C) subdural hygromas post ETV demonstrated on T2 axial MRI.")
Fig. 10:
Three different patients with right (A), left (B), and bilateral (C) subdural...
 is axial non enhanced axial CT showing right intraventricular hemorrhage (red arrow) and left penumocephalus (blue arrow). Second (B) T2 axial MRI showing right penumoventricle (yellow arrow) and small bilateral intraventricular hemorrhage. (C) axial GRE demonstrate blooming of the brain parenchyma about the lateral ventricles bilaterally, consistent with blood products.")
Fig. 12:
Post ETV evaluation of three different patients. The first (A) is axial non...

Fig. 14:
Right subdural hematoma post ETV seen on T2 axial MRI.
, SPACE (middle), and phase contrast (right) sequences in the same patient.")
Fig. 9:
Visual comparison of flow as detected on the CISS (left), SPACE (middle), and...

Fig. 6:
Cine phase contrast sequence in the sagittal plane demonstrating functional...

Fig. 7:
Cine phase contrast sequence in the sagittal plane demonstrating functional...

Fig. 8:
Cine phase contrast sequence in the axial plane demonstrating functional flow...

Fig. 17:
SSFP MR image showing normal appearance of the bilateral trigeminal nerves
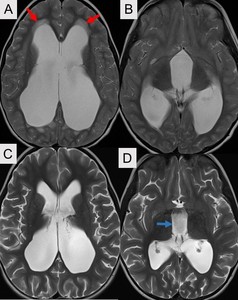
 are pre-operative and show moderate to severe triventricular upstream hydrocephalus with transependymal flow (red arrows). Post operative MRI (Panels C and D) show interval decrease in prominence of the third and lateral ventricles. Note the flow voids in third ventricle (blue arrow) related to flow through the ostomy. The tranependymal flow has resolved.")
Fig. 3:
T2 weighted axial MRI images. Panels (A and B) are pre-operative and show...
 showing diffuse meningeal enhancement (yellow arrow) which can bee seen with meningitis. There is also evidence of ventriculitis (red arrows) including ependymal enhancement (A) and diffusion restriction (B) in the left occipital and atrial region of the lateral ventricle.")
Fig. 11:
Post contrast T1 axial MRI (A) showing diffuse meningeal enhancement (yellow...

Fig. 16:
SSFP MR image at the level of the pontomedullary junction shows normal...

Fig. 15:
Panel A and B show normal appearance of the fornix on Coronal T2 WI and...